
 MERYL NASS, M.D., merylnass at gmail.com, @NassMeryl
MERYL NASS, M.D., merylnass at gmail.com, @NassMeryl
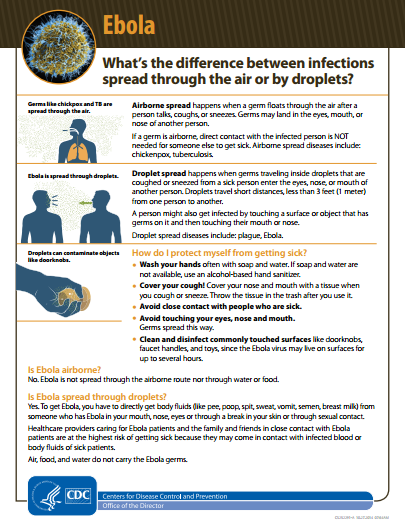
Nass writes at the Anthrax Vaccine blog. She said today: “After months of loudly claiming that Ebola can’t spread through the air [eg, ‘Ebola is not spread through the air or by water‘], late Friday the CDC finally put out an infographic somewhat forthrightly acknowledging air droplet transmission of the disease [PDF].
“The graphic states that ‘Ebola is spread through droplets’ and ‘droplets can contaminate objects like doorknobs.’ CDC attempts to split hairs by the way it contrasts such transmission with ‘airborne’ transmission, and the CDC is insisting that such transmission occurs no further than three feet from the affected patient — while there’s good evidence small droplets may travel much further, and remain viable (infectious) on surfaces for hours or sometimes days.
“The CDC’s stance on droplets was part of a pattern: saying Ebola could be ‘stopped in its tracks’ in the U.S., and that U.S. hospitals are ready.
“Unfortunately, U.S. hospitals are not ready. Anthony Fauci of the NIH recently said: ‘We need to have more than just the four [biocontainment units] in which you have people who are pre-trained…’ It’s certainly true we need more than the current four Biosafety Level 4 centers for the entire U.S., but it’s not just a matter of training. They have facilities other hospitals — including Bellevue — just don’t have. Both Dr. Craig Spencer and patient Thomas Eric Duncan have been treated in emptied, isolation wards. What happens when there are too many Ebola patients to be treated in otherwise empty ICUs, by armies of healthcare professionals?
“The way Bellevue is responding to Ebola is just not sustainable for a large epidemic. The isolation rooms cost $3-4 million each to create.” See: Wall Street Journal: “Bellevue, Home to Ebola Unit, Moves Patients to NYU.” The Daily News reports: “Dozens of specially trained staff are required to man Bellevue’s Ebola ward, which is on the seventh floor and has four beds. And with some 20 nurses and ancillary staff rolling through during a 24-hour shift, that meant pulling staff from the 10th floor ICU.”
Nass adds: “There are a host of huge issues we should be dealing with, including: The slowness and sheer paltriness of the international response in Africa; the $60 plus billion that was supposed to be spent (since the anthrax letters in 2001) to get vaccines and drugs for ‘Category A’ threats including Ebola; the accidental release of viruses from labs and the intentional creation of more dangerous viruses at U.S. bioweapons labs, aka ‘gain of function’ research.”
See IPA news release from Oct. 21: “Ebola: Are U.S. Bioweapons Labs the Solution, or the Problem?” New York Times from Oct. 17: “White House to Cut Funding for Risky Biological Study” and USA Today from Aug. 17: “Hundreds of Bioterror Lab Mishaps Cloaked in Secrecy.”
See past posts by Nass:
“CDC now admits Ebola can float through the air, and land on doorknobs.”
“Ebola Causes Chronic Illnesses in Those Who Manage to Recover/ CBS and USAMRIID.”
“Indemnifying Pharma for Ebola Vaccines: Recipe for Problems?”
“Airborne Spread of Ebola from Pigs to Macaques / Nature.”
“CDC defined infectious respiratory droplet transmission as different than airborne.”